What is Adolescent Idiopathic Scoliosis?
Adolescent idiopathic scoliosis (AIS) is a curvature of the spine that appears around the onset of puberty. Idiopathic means we don’t know why the scoliosis started. Scoliosis causes the spine to curve toward one side. The spine also twists, or rotates, and as the spine twists the ribs move with it. If the curvature is small, it is usually not noticeable except on an x-ray and does not require any treatment.

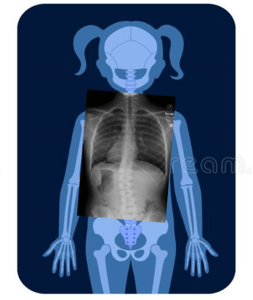
Girl without scoliosis. Her Cobb angle measures 0 degrees.
Girl with mild scoliosis. Her Cobb angle measures 25 degrees.
What Happens without Treatment?
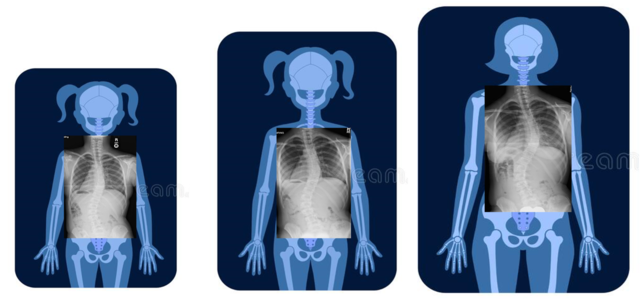
This girl has 2 curves. On the left, she is 11 and her curves measure 34 and 42 degrees. 2 years later, her scoliosis has progressed and the curves measure 40 and 42 degrees. When she’s 18, the curves have continued to worsen to 52 and 53 degrees.
- Curves can continue to get bigger (progress) throughout adulthood, especially if the curve is larger (>50 degrees) when you’re done growing. That’s why many doctors talk about surgery at this point.
- AIS usually causes no other health problems, and people with AIS get along much like others their age. AIS usually has no effect on pregnancy and childbirth. AIS is not associated with higher rates of disability or death.
- Patients with AIS may have more back pain, but this does not seem to be related to the size of the curve.
- If the curve is large (>50 degrees) and in the thoracic (chest) area, then patients may notice some decrease in lung functioning and may have shortness of breath with activities.
- People react to having scoliosis differently, and it’s hard to predict if it will affect your self-image, social interactions, or perception of your health. These reactions do not seem to be related to the size of the curve.
Why is Surgery Sometimes Recommended?
Your doctor might talk about surgery with you for these reasons:
- Your curvature measures more than 45 degrees AND you are still growing. This may mean that your curve will continue to get worse throughout adulthood.
- You have back pain related to your curvature that doesn’t get better with physical therapy or other non-surgical treatments.
- You are very unhappy with the way your back makes you feel.
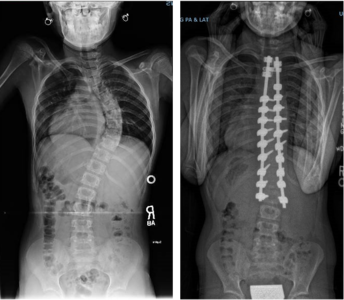
The most common surgery for scoliosis is spinal fusion and instrumentation.
- Surgery involves using metal screws and rods to make the spine straighter. Some of the vertebrae are fused (grow together) to keep the spine in the straightened position.
- Current surgical techniques are safe and effective. However, this surgery is a major procedure and there are risks involved. Some of these risks include heart or lung problems, bleeding, infection, nerve problems and the need for further surgery. Patients are usually in the hospital for 3-4 days, and then might need to limit their activities for the first few months. By 6-8 months, when the fusion is healed, patients can go back to all their usual activities.
- Most patients are very happy with the results, although some may not like the look of the scar, or the fact that their spine is still not completely straight, or that their shoulders, back and hips are still not completely level. Since some of the spine is fused, patients may have decreased motion in their backs.
- Because surgery is a MAJOR undertaking, most patients and doctors consider it a priority to keep curves as small as possible and out of surgical range.
Treatments Considered by BrAIST-Calc:
Observation
Observation, or watching and waiting, consists of follow-up visits and x-rays on a regular basis so the doctor can watch the curve and see if it changes. The doctor will keep you informed about any changes, and if it appears that the curve is getting bigger, then you can discuss what to do next. Observation is used for curves below 20 - 25 degrees or for patients who are done growing. In the BrAIST study, 42% of patients who were observed DID NOT progress to 50 degrees while they were still growing. This means that not everyone needs to wear a brace to avoid progression to surgery.
-
Why might you like observation?
- You wouldn’t have to wear a brace
- You would not have to change your activities
- There are no foreseeable side-effects
- You would not have worn a brace unnecessarily if your curve does not progress
-
Why might you NOT like observation?
- You and your parents may feel like you’re not doing anything to treat the curve
- Bracing may not work if you start it later after your curve has gotten worse
- Your curve might progress to the point where your doctor recommends surgery
- If your curve gets worse, you may feel bad because you didn’t try a brace
Treatments Considered by BrAIST-Calc:
Bracing
Bracing has been used for the prevention of curve progression for many years and is recommended for patients with scoliosis that measures 20-45 degrees AND who are still growing. Most patients wear the brace until they become skeletally mature and stop growing. Depending on how much growth you have left, you could wear a brace 1, 2 or 3 years. Bracing is stopped when you are finished growing -or- when you and your doctor agree that bracing is not working. If the curve is large (>45 degrees) the next step may be a discussion of the risks and benefits of surgery.
-
How do I get a brace?
- The doctor or nurse will send you to see an orthotist. Orthotists are the professionals who make and fit braces.
- The braces we use today are usually made of plastic and fit like a shell around your torso. Braces are custom-made to fit your body.
- First, the orthotist measures you. They may use a tape measure, a cast, or a scanner and a computer program to determine your measurements and the shape of your trunk.
- Braces work by pushing on the ribs or the muscles in the lower back to straighten the spine. The brace is designed to push exactly where you need it. Straightening the spine may help the vertebrae grow more normally and keep the curvature from getting worse.
- Braces come with different names and different designs, including Boston, Rosenberger, Wilmington, Rigo-Cheneau type, Providence, etc. There is no research showing that one type of brace is better than another. The important thing is that the brace fits comfortably, corrects your curve, and that you wear it.
- Doctors usually prescribe 16-23 hours of brace wear a day. You can take the brace off for sports and other physical activities.
- You will see the doctor or nurse and the orthotist on a regular basis for examinations and x-rays. If the brace becomes too small, it needs to be adjusted or replaced.
-
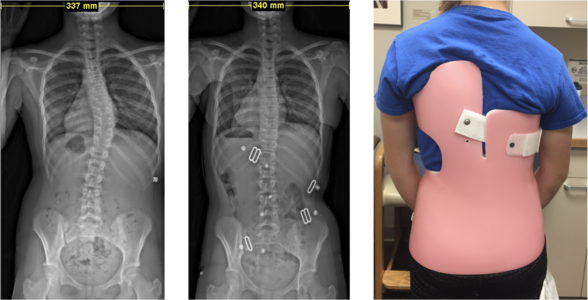
Here are x-rays of a girl before she got a brace and of her in the brace.
-
What might you like about a brace?
- You and your parents may feel that you’re taking control of your scoliosis and doing your best to promote your health.
- Wearing a brace may keep your curve from progressing to the point where surgery is suggested.
-
What might you NOT like about a brace?
- Wearing a brace may interfere with your usual activities, especially if you need to wear it for most of the day.
- It may be important to you to find clothes that cover your brace. These clothes may be different from the ones you normally wear.
- You and your parents might disagree about when and where you wear your brace.
- Even though you wear your brace like you’re supposed to, there’s still a possibility that your curve will progress to the point where the doctor suggests surgery.
-
Here are x-rays of a girl before she got a brace and of her in the brace.